
Treatment journey
From Diagnosis to Treatment Journey
Going through treatment for neuroblastoma can feel overwhelming, but understanding what lies ahead can help families feel more prepared and empowered.
Frist steps after diagnosis
The diagnosis of neuroblastoma in your child is news that brings many questions, worries, and uncertainties. You are facing a challenging time in which you will get a lot of information.
Your child will be treated and cared for by many specialists such as pediatric oncologists, surgeons, radiation therapists, but also neuropsychologists, teachers, physiotherapists, occupational therapists, speech therapists, and others. They all form the treatment team together. This ensures that your child receives comprehensive care from all sides.
Treatment begins as soon as the tumor has been precisely located and characterized. The approach depends on the child's age, the type of tumor, its location, possible metastases, and certain genetic alterations. If the tumor has not metastasized and shows no aggressive genetic changes, surgery is often sufficient. If the tumor is not immediately operable, it is first shrunk with chemotherapy and then, if necessary, removed. In case of metastases or specific genetic alterations, more intensive treatment is required. This includes chemotherapy, surgery, radiation therapy, high-dose chemotherapy with stem cell transplantation and immunotherapy. In some cases, for example, small tumors in newborns that do not interfere with the child´s well-being, the doctors might watch your child carefully without treatment and see if the tumor disappears on its own.
Your doctor will talk to you about the necessary treatment and will also explain the risks and side effects.
A Hickman catheter is usually implanted before the start of treatment. This is a plastic tube that is inserted into one of the major blood vessels under anesthesia and grows into a tunnel in the skin. Usually, two branches protrude from the skin, though in young children sometimes only one. Using this catheter, doctors can administer cytostatic drugs and draw blood without having to search for a blood vessel each time. Puncture is not necessary, but the tube must be flushed regularly.
Phases of treatment
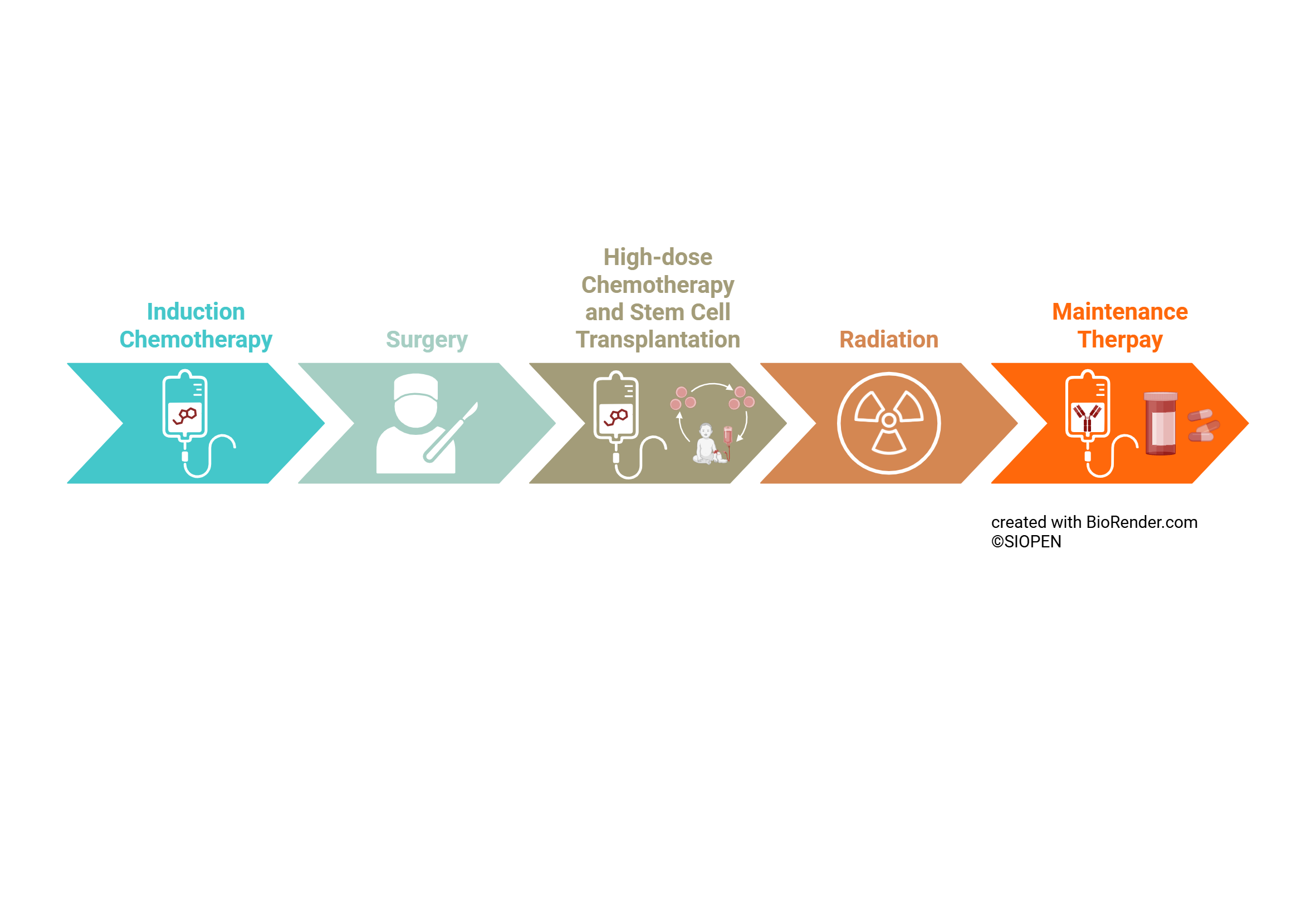
Chemotherapy
Many children with neuroblastoma need chemotherapy as part of their neuroblastoma treatment. In most cases, the neuroblastoma is not operable in the beginning and chemotherapy is used to shrink the tumor.
Chemotherapy is a treatment with medications (cytostatics) that inhibit cell division. This kills tumor cells, inhibits tumor growth, and attacks possible metastases. To fight the tumor as effectively as possible, your child will receive a combination of several cytostatic drugs.
The following medications are most effective for neuroblastoma: carboplatin, cisplatin, cyclophosphamide, doxorubicin, etoposide, topotecan, vincristine, and irinotecan. The treatment protocol details exactly what medication your child will receive and when.
Your doctor will explain the schedule and possible side effects to you: Besides their desired effect on tumor cells, cytostatic drugs also affect your child's blood cells, mucous membranes, skin, and hair. As a result, nausea, fatigue, mouth pain, loss of appetite, and hair loss can occur. Furthermore, your child's weakened immune system makes them particularly susceptible to infections. Although these side effects disappear after treatment, they are very unpleasant and can significantly impact your child's life.
Often, supportive treatment in the form of medication, blood transfusions, and sometimes feeding via a gastric tube is necessary.
Surgery
The timing of surgery depends on tumor localization and disease stage. Some tumors are operable at diagnosis, for most of the tumors however surgery will be done in the course of the treatment.
Before the operation, the pediatric surgeons will explain to you and your child what will happen. The goal is to remove the tumor as completely as possible. Often, however, this is not possible due to the tumor's location close to blood vessels and organs, leaving behind some small tumor rests.
During the operation, the entire area will be thoroughly examined, and as many suspicious areas as possible will be removed. Often, due to the tumor's growth, an adrenal gland or part of the sympathetic trunk must also be removed. The kidney can mostly be preserved.
After the operation, pathologists will examine the tissue to check how much of the tumor has died as a result of the therapy. Based on these findings and the data from other examinations, further treatment will be determined. Your child will be prepared for the operation by trained staff.
Removing a tumor is a major procedure and can take several hours. Your child will stay in the care of the pediatric surgery team for a couple of days and will be observed for possible complications following the surgery.
Apheresis and Re-Infusion of Stem Cells following High-dose chemotherapy
High-dose chemotherapy may be necessary to destroy even the smallest, invisible tumor cells. Because this puts a heavy strain on the bone marrow, stem cells are extracted from the blood beforehand (apheresis) and later reinfused (re-infusion).
After chemotherapy, your child will receive a small daily injection of a growth factor (G-CSF) to help mobilize stem cells from the bone marrow into the bloodstream. This can temporarily cause flu-like symptoms or bone pain – paracetamol often helps with this.
After one to two weeks, the stem cells are filtered from the blood. For this procedure, your child will have IV lines inserted in both arms, through which the blood is drawn and passed through a special device that collects the stem cells. The extraction takes about four hours and can be repeated the following day if necessary. The stem cells are frozen until needed.
After completion of high-dose chemotherapy, the patient's own stem cells are returned via infusion, just like a blood transfusion. They settle in the bone marrow and ensure that the bone marrow functions normally again and regenerates more quickly.
Radiation therapy
Radiation therapy kills tumor cells and inhibits their growth.
It is recommended for patients with metastatic tumors and/or more aggressive tumors, as well as for older children after chemotherapy for localized tumors. The area where the tumor was removed is typically irradiated.
To achieve the greatest possible effect without too many side effects on the healthy surrounding tissue, the radiation is administered over several weeks, with your child receiving a short, daily treatment lasting only a few minutes. The amount of radiation your child will receive will be determined in advance, and the treatment area will be precisely marked. Healthy body parts will be protected as much as possible and covered with lead aprons.
Proper preparation for the treatment is extremely important for your child. Radiation therapy is invisible and inaudible; your child will not feel a thing. However, it can be an uncomfortable experience, as your child will be lying alone in a large room under a large machine. You will be standing behind a thick wall, maintaining contact with your child via a monitor and/or an intercom. For younger children, the radiation treatment is administered under brief sedation (twilight sleep) to ensure they remain completely still. Ask what you can do to best support your child during this time. Sometimes playing music or reading to your child via the intercom can be helpful.
Maintenance
In many patients with neuroblastoma, your doctors will recommend maintenance therapy, which aims to kill or mature remnant tumor cells and prevent relapse. Possible medications are isotretinoin and immunotherapy with antibodies.
Isotretinoin
is a form of vitamin A that inhibits the growth of neuroblastoma cells, though it is only effective when minimal residual tumour cells remain. In high-risk tumors, vitamin A is used at the end of treatment alongside immunotherapy to promote the maturation of any remaining tumor cells.
For localized tumors, vitamin A therapy is sometimes recommended for six months after the end of chemotherapy. A high dosage is required for optimal effectiveness, but this can unfortunately cause unpleasant side effects such as red, dry, and itchy skin, chapped lips and gastrointestinal problems. Ask your doctor what can be done about these side effects.
Immunotherapy
Dinutuximab is an immunotherapy drug used in combination with isotretinoin to prevent neuroblastoma relapse. It is a monoclonal antibody that targets the GD2 molecule on neuroblastoma cells, signalling the immune system to destroy them. Dinutuximab is given for 10 days as a continuous infusion every 5 weeks for 5 cycles.
The most common and significant side effect is neuropathic pain, which is managed with strong pain medications. Usually, the body gets used to this side effect over some days, and your child will need less or no pain medication within one cycle and with the following cycles. Other side effects are fever reactions, low blood pressure and itching rash.
What to expect during hospital stays
While some chemotherapies can be given in outpatient clinics, for most of the neuroblastoma chemotherapies, your child will have to be admitted to the hospital for a couple of days (depending on the chemotherapy cycle). Your child will be on a ward that is specialized on pediatric oncology, so doctors, nurses and all other staff are experienced in the administration and the side effects of the medications.
During chemotherapy, and maybe some days after, your child might feel nauseous and throw up, your doctors will prescribe medications to prevent this. Some medications could cause allergic reactions and your child needs to be monitored closely during the infusion. Usually, your child will receive intravenous fluids during chemotherapy and the amount of urine will have to be measured to ensure that all given fluids are excreted via the kidneys.
Depending on the treatment, regular blood draws may be needed to monitor various body functions and immune system health. If needed, your child may also receive blood transfusions to help the body recover from the medication toxicities. All these infusions are usually done through the child’s IV line without having to poke them regularly.
Between chemotherapy cycles, your child might develop a fever – it is crucial that you inform your doctors and come to the hospital right away, as your child’s immune system is compromised after chemotherapy and infections could become dangerous. In most cases of fever, your child will be admitted for antibiotic treatment.
Sometimes the mucous membranes are inflamed and you child needs treatment to control pain.
In most cases, one of the parents can stay with their child around the clock. Most pediatric oncology departments offer playrooms and different activities so that time goes by faster.
SIOPEN Clinical Trials
SIOPEN coordinates a number of clinical trials for children and young people with neuroblastoma.
Clinical trials are studies that look at how treatments work and help doctors improve care. On the webpage, you can find information about the SIOPEN trials that are currently open, what they involve, and who may be able to take part.
If you are thinking about a clinical trial, it is important to talk with your child’s medical team. They can help you understand whether a study might be suitable for your child and answer any questions you may have.
Glossary of common terms in paediatric oncology
Adrenal Glands
Small hormone-producing glands that sit on top of each kidney.
The adrenal glands help control heart rate, blood pressure, stress response, and other important body functions. Neuroblastoma often starts in these glands.
Biopsy
A small sample of tissue is taken from the body to be examined under a microscope.
Doctors perform a biopsy to confirm whether a tumour is cancer and to learn more about its specific features, which helps guide treatment.
Bone Marrow
The soft, spongy tissue inside bones where blood cells are made.
Bone marrow produces red blood cells (carry oxygen), white blood cells (fight infection), and platelets (help stop bleeding).
Neuroblastoma can sometimes spread to the bone marrow.
Extracranial
Outside of the brain.
If a tumour is extracranial, it means it is located somewhere in the body other than the brain.
Horner’s Syndrome
A group of symptoms caused by pressure or damage to certain nerves in the neck.
It can cause:
A drooping eyelid
A smaller pupil in one eye
Reduced sweating on one side of the face
In neuroblastoma, this can happen if a tumour presses on nearby nerves.
CT Scan (Computed Tomography)
A detailed X-ray scan that creates cross-section pictures of the body.
A CT scan helps doctors see the size and location of a tumour and whether it is pressing on nearby organs.
MRI (Magnetic Resonance Imaging)
A scan that uses magnets and radio waves to create detailed pictures of the inside of the body.
An MRI does not use radiation. It helps doctors see tumours, nerves, and soft tissues clearly.
PET scan (Positron Emission Tomography)
A scan that shows how active cells are inside the body.
A small amount of a safe radioactive sugar solution is injected into the bloodstream. Cancer cells often use more sugar than normal cells, so they “light up” on the scan.
Metastasis
When cancer cells spread from the original (primary) tumour to other parts of the body.
These cells travel through the blood or lymph system and form new tumours elsewhere.
Paraspinal Nerve Tissue
Nerve tissue located next to the spine.
“Paraspinal” means beside the spine. Neuroblastoma often develops from early nerve cells that run along the spine.
Treatment-related terms in Pediatric Oncology
Central Line (Port)
A small tube is placed into a large vein to give medicines and take blood without repeated needle sticks.
Chemotherapy
Medicines that kill cancer cells or stop them from growing.
Immunotherapy
Treatment that helps the body’s immune system find and attack cancer cells.
Radiation Therapy
High-energy rays used to destroy cancer cells.
Relapse / Recurrence
When cancer comes back after treatment.
Remission
When signs of cancer decrease or disappear after treatment.
Side Effects
Unwanted effects of treatment, such as nausea, hair loss, or infection risk.
Stem Cell Transplant
A treatment where a child receives high-dose chemotherapy followed by replacement of blood-forming stem cells.
Surgery
An operation to remove as much of the tumour as possible.